Joseph Nguyen
Abstract
Hypothesis: Opiates mediate pain via opioid receptors, which consist of several subtypes. One subtype, the kappa opioid receptors (KOR), has also been shown to prevent addictive behaviour. Potential novel therapeutic compounds acting on KOR include U50488, CR665, and CR845. It is hypothesized that selective kappa opioid receptor agonists are effective at controlling pain while managing opioid addiction.
Methods: Studies for this review were obtained through the PubMed database using a keyword search strategy. Only articles in English published from December 2006 until December 2016 were considered.
Results: Kappa agonists are able to decrease inflammatory, visceral, and surgical pain, but are unable to inhibit behaviour-depressing aspects of pain. Kappa agonists also decrease field potential and long-term potentiation in the basolateral amygdala. Additive anti-nociception with mu opioids has been observed as well as decreased fentanyl use, morphine tolerance development, and morphine withdrawal symptoms.
Conclusions: Kappa agonists can be effective analgesics while also preventing abuse and addiction to mu opioids. Some evidence also suggests kappa agonist activity in the basolateral amygdala can inhibit affective components of pain.
Abstract Word Count: 175
Keywords: kappa agonist, pain, analgesia, anti-nociception, tolerance, dependence, withdrawal, addiction
Ultramini Abstract: This study reviewed current research on the analgesic and anti-addictive properties of selective kappa agonists for their use in pain management while preventing addiction.
Introduction
Opioids are one of the most powerful analgesics available with an increasing trend of prescription in the United States. Prescriptions per capita increased 7.3% from 2007-2012 with 259 million prescriptions in 2012, enough for one bottle of opioids per adult (Dowell et al., 2016). On the other hand, use of opioids presents risks including dependence, abuse, addiction, and overdose which lead to negative health, social and economically impacts. From 1999 to 2014, over 165,000 people have died from opioid overdose and in 2013; an estimated 1.9 million people abused or were dependent on prescribed opioids (Dowell, Haegerich & Chou, 2016). However, pain treatment should not be ignored as “there are clinical, psychological, and social consequences associated with chronic pain including limitations in complex activities, lost work productivity, reduced quality of life, and stigma, emphasizing the importance of appropriate and compassionate patient care” (Dowell et al., 2016).
The CDC has recently released a guideline, aimed at primary care settings, suggesting prescriptive protocols as well as methods to evaluate risk of patient substance abuse and addiction. However, the majority of evidence reviewed by the guideline had significant limitations. Although the CDC guideline still has value in preventing exacerbation of pre-existing risk of abuse, results and implementation remain to be seen.
Efforts have been made to deter abuse through novel drug formulations, barriers, and pharmacokinetics. Nevertheless, nothing can prevent an addicted person from taking multiple doses at once. This may be a result of the inherent nature of the drugs to activate reward pathways in the brain along with its analgesic effects though mu receptors. Another opioid receptor, kappa-opioid receptor (KOR), has been shown to “limit motivational properties of drug abuse” (Lalanne, Ayranci, Keiffer & Lutz, 2014). This has sparked interest in development of kappa agonists as novel analgesics with low abuse potential. Examples of known selective kappa agonists include U50488, CR665, and CR845 among many others including those continuing to be developed. However, questions still remain about analgesic efficacy and complications for patients already addicted to mu opioids transitioning to kappa agonists. This literature review explores the anti-nociceptive efficacy of kappa agonists and their ability to manage opioid addicted patients.
Balancing adequate pain control with risk of future abuse has been a difficult endeavour for physicians as well as patients. This topic was chosen to investigate the possibility of a potent pain medication without addictive properties as an alternative to traditional mu opioids. Surely, this would be a major instrument in the treatment of chronic pain. This study will be done under the hypothesis that kappa agonists are effective in management of pain and opioid addiction.
Methods
A search was performed for published literature on PubMed. Search terms were selected to assess analgesic properties and anti-addiction properties of kappa agonists on opiate use (Table 1). The search terms used included: pain, chronic pain, kappa opioid, kappa agonist, pain control, anti-nociception, withdrawal, dependence, addiction, and tolerance. This study looked at articles in English published between December 2006 and December 2016. Articles of all levels of evidence were considered and included review, preclinical, and clinical data. The initial search produced 574 results. These resources were then screened with the following exclusion criteria: articles not involving kappa agonists/receptors, articles on opioids without kappa receptor selectivity, articles on opioids with dual agonist activity, articles on kappa agonist interaction with drugs that were not analgesics. Abstract reviews of the remaining articles were performed to select for articles on analgesic efficacy or anti-addictive properties of selective kappa agonists. The resulting collection of evidence was organized into an evidence table (Appendix).
Table 1-Keyword Search Strategy
|
Population |
Intervention |
Comparison |
Outcome |
|
Pain OR Chronic Pain |
Kappa opioid OR Kappa agonist |
Analgesia OR Analgesic OR Pain control OR Antinociception OR Anti-nociception OR Withdrawal OR Dependence OR Addiction OR Tolerance |
Results
A final total of 11 articles were included in this study, the majority being animal studies on mice or rats. One study involved rhesus monkeys. There was one study that involved a human clinical trial. Also, there was one review using human clinical trials focused only on peripherally selective kappa agonists.
Table 2-Summary of Study Designs Reviewed
|
Study Design |
# of Studies |
|
Animal Models |
9 |
|
Clinical Trials |
1 |
|
Review |
1 |
Analgesic Efficacy
An animal study by Auh and Ro (2012) induced inflammation in rat hindpaws with injections of complete Freund’s adjuvant. After 3 days, when mechanical hyperalgesia was well developed, local injections of kappa agonist U50488 were given at different doses and mechanical threshold for hindpaw withdraw response was measured. The results showed dose-dependent increase in mechanical threshold by local injections of U50488 (Auh & Ro, 2012). A time effect was also observed where increasing doses of U50488 prolonged the anti-hyperalgesia effect.
The role of kappa opioids in inflammatory pain was also studied by Moon et al. (2016) in a research on the effects of peripheral kappa opioid receptors and arthritic pain. Arthritis was induced in rats using 1% λ-carrageenan injected into the knee. After nociceptive behaviour was maximally expressed (reduced weight-bearing in ipsilateral joint), U50488 was injected into affected joints. A two-way repeated-measure ANOVA showed significant recovery of reduced weight-bearing in the affected limb in comparison to saline. In addition to inhibited nociceptive behaviour, U50488 was also found to reduce mechanosensitive afferent nerve fibre activity in the carrageenan-induced inflamed knee using nerve recording techniques.
Aside from inflammatory pain relief by U50488, the peripheral kappa opioid CR665 was found to significantly increase pain threshold to esophageal distension in a study by Arendt-Nielsen et al. (2009). This randomized, double blinded, controlled study compared the effects of CR665 against oxycodone on skin, muscle, and visceral pain stimulation in healthy males. Although CR665 increased pain threshold to esophageal distension, oxycodone had the same effect with addition to increased pain threshold to cutaneous pinch pain, cuff pressure pain, and thermal stimulation.
A number of other clinical trials, on peripheral kappa agonist CR845, were reviewed by Albert-Vartanian et al. (2016). A randomized, double-blinded, placebo-controlled study was conducted on elective hysterectomy patients for analgesic efficacy before and after the procedure, using a 10 cm visual analog scale for measurement of pain intensity. If pain persisted after 24 hours, rescue medication (IV morphine) was given. Significant differences were observed in comparison to patients who only received placebo. Less use of rescue medication as well as a 2-fold decrease in pain intensity was found in patients that received CR845 before and after the surgery.
Albert-Vartanian et al. (2016) also discussed a phase 2, randomized, double-blinded, placebo-controlled clinical trial in patients electing bunionectomy surgery with fentanyl as rescue medication. Over a 48 hour period, pain was measured regularly using a visual analog scale. The study used a sum of pain intensity difference from baseline levels over 24 hours (SPID0-24) as a measurement for efficacy along with SPID0-36 and SPID0-48. In patients who completed the study, there was a statistically significant reduction in SPID0-24 and SPID0-48 in those treated with CR845 compared to placebo. However, there was no significant difference in the modified intent-to-treat group.
In another phase 2 trial, patients with moderate to severe osteoarthritis pain (>4 out of an 11 point scale) were given an oral form of CR845 with acetaminophen as a rescue drug over 2 weeks (Albert-Vartanian, 2016). A dose-dependent reduction in average pain score of 25-34% was observed. Among patients receiving the highest dose of CR845, 50% had a reduction of ‰¥30% in their reported pain score at the end of the 2 weeks with an 80% reduction in requirement for acetaminophen.
Analgesic Efficacy with Other Measures of Pain
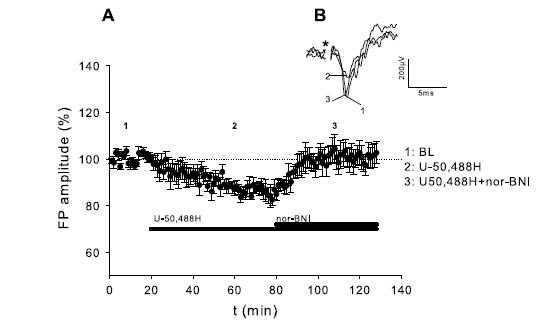
Aside from sensory components of pain, there are affective and behavioural components of pain as well. An electrophysiological experiment conducted by Huge, Rammes, Beyer, Zieglgansberger, & Azad (2009) looked at the effects of kappa opioid receptors activation on mice basolateral amygdala, an area of the brain that is involved in pain processing and pain memory formation. The field potential amplitudes were measured at baseline and under induced long-term potentiation using high frequency stimulation and the effects of kappa agonist U50488H were studied. The experiment found that U50488H decreased baseline levels of field potential amplitude as seen in Figure 1, while these effects were inhibited by kappa receptor antagonist norbinaltorphimine (nor-BNI).
Figure 1. Effects of Kappa Agonist and Antagonist on Field Potential Amplitude of Mice Amygdala. Baseline (BL): 100±0.5%; U50488H: 86.3±2.4%, nor-BNI: 100±4.2%. Data points show average field potential (FP) ± Standard Error. Reproduced from Huge et al., 2009, p. 125.
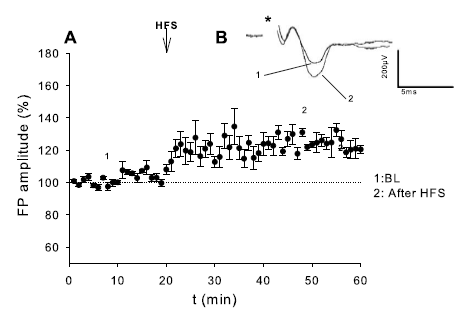
Prior application of U50488H before high frequency stimulation was also found to inhibit induction of long term potentiation (Figure 2) in comparison to long term potentiation induction with no drug (Figure 3).
Figure 2. Effect of Kappa Agonist Pre-treatment on High Frequency Stimulated Long Term Potentiation of Mice Amygdala. U50488H: 100±4.1%; High Frequency Stimulation (HFS): 102.6±7%. Data points show average field potential (FP) ± Standard Error. Reproduced from Huge et al., 2009, p. 126.
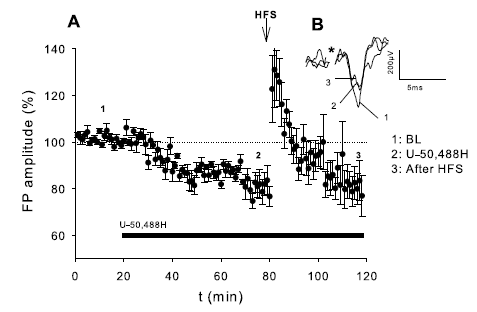
Figure 3. Long Term Potentiation Produced by High Frequency Stimulation. Baseline (BL): 100±2%, High Frequency Stimulation (HFS): 119±4%. Data points show average field potential (FP) ± Standard Error. Reproduced from Huge et al., 2009, p. 126.
Although pain-stimulated behaviours are often used as a measure of pain, such as a withdrawal or writhing response, complementary measures are behaviours that diminish in the presence of pain stimuli (Negus, O’Connell, Morrissey, Cheng & Rice, 2011, p. 506-507). An experiment by Negus et al. (2011) studied the effects of peripheral and central kappa agonists compared to ketoprofen on rats trained to evoke intracranial self-stimulation using a lever, a behaviour that is depressed by pain. Intraperitoneal lactic acid injection acted as a pain-inducing stimulus, with a stretch response being a pain-stimulated behaviour to contrast with the pain-depressed behaviour of intracranial self-stimulation. It was found that the central kappa agonist (salvinorin A), peripheral kappa agonists (ffir and ICI204448), and ketoprofen all inhibited lactic acid induced stretching. However, only ketoprofen inhibited lactic acid induced depression of intracranial self-stimulation. Salvinorin A had actually increased depression of intracranial self-stimulation while ffir and ICI204448 had no appreciable effect.
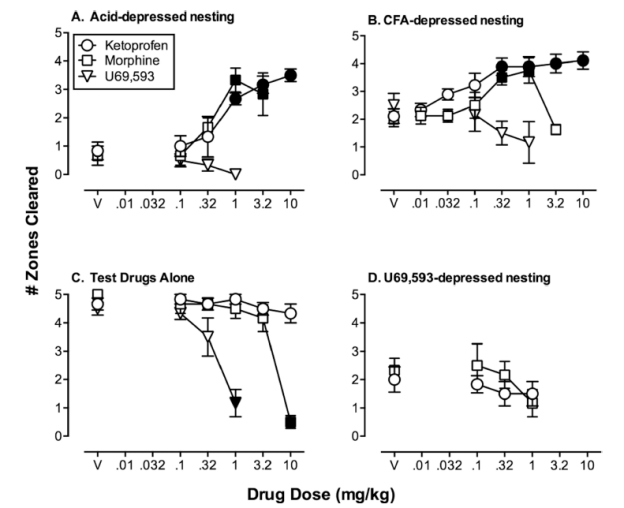
Similar results were found when Negus et al. used depression of nesting in mice as a measure of pain (2015). Kappa agonist U69593 failed to both inhibit and reverse depression of nesting induced by intraperitoneal lactic acid and intraplantar complete Freund’s adjuvant (Figure 4A & 4B). However, 1-way ANOVA analysis (p<0.001) showed that both ketoprofen and morphine prevented, as well as reversed, depression of nesting in a dose-dependent manner (Figure 4A & 4B). U69593 was shown to actually depress nesting when administered independently (Figure 4C) and this effect was not able to be reversed by neither ketoprofen nor morphine (Figure 4D).
Figure 4. Effects of Ketoprofen, Morphine, and U69593 on Nesting under Different Conditions. Panel A: Nesting depressed by intraperitoneal administration of 0.32% lactic acid. Panel B: Nesting depressed by intraplantar administration of complete Freund’s adjuvant. Panel C: Nesting under no treatment. Panel D: Nesting depressed by U69593. Nesting represented as the number of zones cleared of nesting material. V represents drug vehicle only. Darkened points represent significant difference from drug vehicle under given condition. Reproduced from Negus et al., 2015, p. 18.
Interactions with Mu Opioids
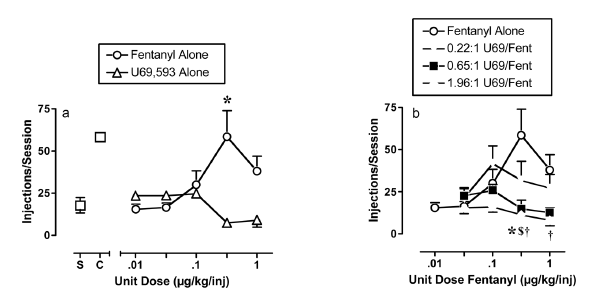
There is evidence suggesting kappa agonists have anti-addictive effects (Lalanne et al., 2014). However, it is important to evaluate the effects of kappa opioids in concurrent use with mu opioids. A study on interactions of fentanyl and U69593 in rhesus monkeys showed a decrease in the rate of drug self-administration when the kappa agonist was added to fentanyl compared to fentanyl alone (Negus, Schrode & Stevenson, 2008). This effect increased with greater proportions of U69593 in the mixture (Figure 5). Using a conditioned response for food as a measurement for activity, both fentanyl and U69593 alone depressed the behaviour while mixtures showed a less than additive effect. Furthermore, at the lowest proportion tested (0.22:1 U69593/fentanyl), U69593 reduced the behaviour depressing effects of fentanyl.
Figure 5. Rate of Self-Administration of Fentanyl vs. Dose of Fentanyl, U69593, or Mixture. Reproduced from Negus et al., 2008.
Negus et al. also demonstrated additive thermal anti-nociception, using tail withdrawal threshold from heated water, with the fentanyl/U69593 mixtures at all proportions tested (2008). More evidence of additive effects of kappa and mu opioids was shown by Sakakihara, Imamachi, & Saito using a similar method in mice (2016). Intrathecal injection of kappa agonist TRK-820 combined with morphine resulted in a stronger anti-nociceptive effect compared to morphine alone. Compared to morphine alone, kappa agonists also have benefits regarding the development of tolerance.
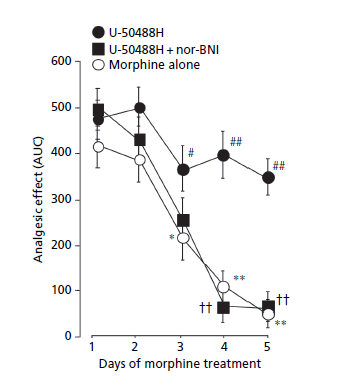
It is well known that repeated use of mu opioids quickly develops tolerance. The addition of a kappa agonist has been shown to inhibit the development of tolerance to morphine (Hamabe, Yamane, Harada & Tokuyama, 2008). Mice treated daily with subcutaneous morphine for 5 days developed reduced analgesia from morphine from days 3 to 5. However, daily administration of kappa agonist U50488H 5 minutes after injection of morphine attenuated the onset of tolerance (Figure 6). Additionally, pre-treatment of kappa receptor antagonist nor-BNI inhibited the tolerance-blocking activity of U50488H.
Figure 6. Effect of Kappa Agonist U50488H on Morphine Tolerance. Each point show means ± standard error. AUC: Area under curve. #: P<0.05, ##: P<0.01 against measurements on day 1. € € : P<0.01 against measurement for U50488H on corresponding day. *: P<0.05, **: P<0.01 against measurement on day 1. Reproduced from Hamabe et al., 2008, p. 1186.
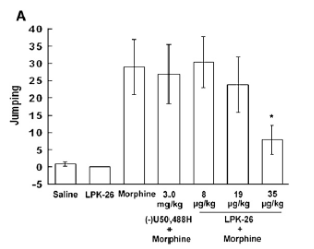
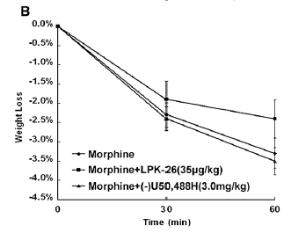
Although U50488H inhibited the development of tolerance it was unable to inhibit morphine withdrawal (Tao et al., 2008). However, Tao et al. demonstrated that another kappa agonist, LPK-26, may be able to. Chronic doses of morphine, kappa agonist (LPK-26 or U50488H), or both were administered to mice over 5 days and induction of withdrawal was achieved by subcutaneous injection of naloxone 2 hours after the final dose of morphine. Chronic treatment with LPK-26 did not produce a withdrawal response. However, chronic treatment with morphine produced a strong withdrawal response in the form of withdrawal jumping. Furthermore, chronic treatment with morphine along with pre-treatment with LPK-26 had a significant reduction in withdrawal response in a dose dependent manner (Figure 7A). Body weight was also measured before and after naloxone withdrawal induction (Figure 7B). Only LPK-26 showed significant reduction of morphine-induced weight loss.
Figure 7. Effects of LPK-26 and U50488H on Withdrawal Jumping and Weight Loss. Data set shown as mean ± standard error. Reproduced from Tao et al., 2008, p.310.
Discussion
Analgesic Efficacy of Kappa Opioids
Side effects of selective kappa agonists mainly stem from its activity in the central nervous system. These side effects are the main hindrance for pharmacologic use of kappa opioids and include dizziness, dysphoria, confusion, sedation, hallucinations, diuresis, and even psychotic symptoms at high doses (Walsh, Strain, Abreu, & Bigelow, 2001). Strategies to minimize these unwanted effects revolve around limiting the activity of kappa agonists to peripheral sites of action. Local injections have been shown to reduce inflammatory pain in animal models through reduced activity of afferent nerve fibres (Auh & Ro, 2012; Moon et al., 2016). Although the analgesic results mentioned were limited to animal models, in humans, intravenous administration of peripherally selective formulation CR665 also shows evidence of analgesia for visceral and surgical pain (Arendt-Nielsen et al., 2009; Albert-Vartanian et al., 2016). Furthermore, oral formulations CR665 have been shown to reduce inflammatory osteoarthritic pain in humans (Albert-Vartanian et al., 2016). Continued pain treatment is required if kappa opioids are to be considered as an alternative to mu opioids and research shows viability of kappa opioids in different formulations and routes of administration for the treatment of pain in traditional measures.
The components of pain include affective elements as well, which is especially important in chronic pain. Pain affect is comprised of the unpleasant emotions associated with pain as well the emotions towards future implications of having chronic pain. The latter is based on reflections of pain memory and is known as secondary pain affect. As a consequence, chronic pain states can lead to depression and anxiety, which lowers well-being and quality of life (Price, 2000). The amygdala is a crucial structure in the brain involved in emotional learning, pain processing, and constructing of pain memories (Huge et al., 2009). Kappa opioids are able to reduce the activity and inhibit long-term potentiation in the basolateral amygdala. As long-term potentiation is considered a cellular model for learning and memory formation, kappa opioids may be able to prevent or extinguish pain memory and treat affective components of pain. However, this experiment, at the moment, is limited to mice and further study is required to assess whether the results can be translated to human. Furthermore, these results may be due to structurally specific central actions on the amygdala as other studies show evidence of dysphoric effects from central kappa opioid receptor activation (Lalanne et al., 2014).
Although kappa agonists have regularly been shown to provide analgesia in assays using pain-stimulated behaviours as measurements of pain, there is contrast when pain-depressed behaviours are observed instead. Pain-depressed behaviours are behaviours that are decreased due to pain. Some examples that have been tested in animal models are feeding, movement, and reinforced behaviours. In humans, it is analogous to mood or functionality. When pain-depressed behaviours are studied, not only do centrally active kappa agonists fail to relieve pain of this aspect, they may worsen it (Negus et al., 2012; Negus et al., 2015). It should be noted that peripherally active kappa agonists relieve pain in pain-stimulated assays without affecting pain in pain-depressed assays and may be safer than centrally active kappa agonists (Negus et al., 2011). In comparison to kappa opioids, conventional analgesics such as mu opioids and nonsteroidal anti-inflammatory drugs do relieve such components of pain in addition to pain-stimulated behaviours (Negus et al., 2011; Negus et al., 2015). Even so, kappa agonist still have value as they have been shown to reduce pain in human trials as discussed previously. The studies on pain-depressed behaviours have limitations to animal models and further studies are needed to understand how clinically relevant the effects may be for humans.
Managing Addiction
Some of the major problems of using mu opioids for pain control are the development of tolerance, dependence, and drug abuse, which may all contribute to addiction. Although there are many other drugs that also relieve pain, the difficulty lies in managing addiction at the same time. Kappa agonists, aside from having low abuse potential, have been shown to decrease self-administration of fentanyl in animal models (Negus et al., 2008). These results are promising evidence for kappa agonists being agents to prevent opioid abuse. Also, kappa agonists have additive analgesic effects with mu opioids (Negus et al., 2008; Sakakihara et al., 2016). This possibly reduces the amount of mu opioid required for effective pain management while also reducing addiction and abuse liability due to less use.
Increased usage of mu opioids may be due to the development of tolerance, requiring increased dosage to maintain analgesia. The high addictive potential of mu opioids makes this a concerning issue. However, addition of kappa agonists during administration of mu opioids may be able to significantly inhibit the development of tolerance (Hamabe et al., 2008). It may be possible to prevent the development of physical dependence and addiction to mu opioids by adding kappa agonists to drug regimens of chronic pain patients.
As for those who are already affected by physical dependence on mu opioids, there is evidence that kappa opioids can inhibit withdrawal symptoms and reduce dependence (Tao et al., 2008). However, some kappa agonists, such as U50488H, do not have any significant effect. It has been suggested that the inconsistency may be due to varying affinities for different subtypes of kappa opioid receptors. Nonetheless, this study demonstrates potential for kappa agonists in managing opioid addiction through modulating dependence and withdrawal. Future studies may provide better understanding on subtype functions and improve designs for desired effects while minimize side effects. Also, as the studies regarding kappa agonist interaction with mu opioids are mainly done on animal models, further investigation is required to see whether results can be extended to humans.
One important point to distinguish is non-selective versus peripherally selective kappa agonists. As mentioned previously, activation of kappa receptors in the central nervous system can lead to many side effects. Peripherally selective kappa agonists still produces analgesia, but it is uncertain whether the effects of the kappa agonists on abuse, tolerance, and dependence are due to central or peripheral activity. If these effects are due to central activity, the benefits of kappa agonists for addiction management will be limited by their undesired side effects. Still, in a study involving a peripherally selective kappa agonist and its effects on nicotine, there is some evidence suggesting that activation of peripheral kappa receptors do inhibit symptoms of withdrawal and dependence by inhibiting activity of central kappa receptors.
Conclusion
In conclusion, this study found that selective kappa agonists provide analgesia to inflammatory, visceral, and surgical pain. In contrast, they were not effective inhibitors of behaviour-depressing effects of pain. Specific activities of kappa receptors in the basolateral amygdala, however, may inhibit affective components of pain. In managing addiction, kappa agonists may able to prevent mu opioid abuse, prevent the development of tolerance, inhibit the symptoms of withdrawal, and reduce physical dependence. The additive effect with mu opioids and the inhibition of tolerance development can reduce the required amount of mu opioids for effective analgesia, thus reducing abuse and addiction likelihood. Overall, selective kappa agonists are a good prospect for managing pain while combating opioid abuse and addiction.
Appendix
Evidence Table
|
First Author |
Date of Publication |
Study Design |
Level of Evidence |
Study Population |
Therapy or Exposure |
Outcome/Results |
|
Albert-Vartanian |
2016 |
Review |
1 |
Human |
CR845 |
CR845 reduced pain with less abuse potential |
|
Arendt-Nielsen |
2009 |
Clinical trial |
1 |
Healthy males |
CR665, Oxycodone |
CR665 is effective on visceral pain |
|
Auh |
2012 |
Animal model |
0 |
Rats |
U-50488 |
Local kappa agonist attenuated inflammatory mechanical hyperalgesia |
|
Hamabe |
2008 |
Animal model |
0 |
Mice |
Morphine, U-50488H |
Analgesic tolerance to morphine is prevented by U-50488H through suppression of PKC |
|
Huge |
2009 |
Animal model |
0 |
Mice |
U-50488H |
Activation of kappa receptors decrease synaptic transmission and long term potentiation in the amygdala |
|
Moon |
2016 |
Animal model |
0 |
Rats |
U-50488, Nor-BNI |
U-50488 inhibits nociception in arthritic knee joints of rats |
|
Negus |
2008 |
Animal Model |
0 |
Rhesus Monkey |
Fentanyl, U69593 |
Addition of kappa agonist to fentanyl demonstrated additive anti-nociception and decreased drug self administration |
|
Negus |
2011 |
Animal Model |
0 |
Rats |
Ffir, ICI204448, Salvinorin A |
Kappa agonists do not inhibit pain-depressed behaviours |
|
Negus |
2015 |
Animal model |
0 |
Mice |
Morphine, Ketoprofen, U69593 |
Morphine/Ketoprofen inhibited pain-depressed behaviours whereas U69593 failed to do so |
|
Sakakihara |
2016 |
Animal Model |
0 |
Mice |
Morphine, TRK-820, Nor-BNI |
Addition of kappa agonist to morphine may have additive anti-nociceptive effects |
|
Tao |
2008 |
Animal Model |
0 |
Mice |
Morphine, LPK-26, U50488H |
LPK-26 is a potent analgesic with low dependence and inhibits morphine withdrawal |
You have to be 100% sure of the quality of your product to give a money-back guarantee. This describes us perfectly. Make sure that this guarantee is totally transparent.
Read moreEach paper is composed from scratch, according to your instructions. It is then checked by our plagiarism-detection software. There is no gap where plagiarism could squeeze in.
Read moreThanks to our free revisions, there is no way for you to be unsatisfied. We will work on your paper until you are completely happy with the result.
Read moreYour email is safe, as we store it according to international data protection rules. Your bank details are secure, as we use only reliable payment systems.
Read moreBy sending us your money, you buy the service we provide. Check out our terms and conditions if you prefer business talks to be laid out in official language.
Read more