microflora in humans regulates numerous bodily processes and cellular functions metabolism, inflammation, immunity, and now has been found to play a role in cancer treatments efficacy, side effects, after effects. talk about the body of the paper. In conclusion, the gut and potentially oral, etc microbiota can be modulated to protect the body from effects of treatment, or even enhance the effectiveness of the treatment.
Introduction
The human body contains numerous microorganisms that inhabit many parts of the body such as the skin, oral mucosa, and gastrointestinal tracts, known as the human microbiota. These microorganisms aid in metabolism, local and systemic immune system responses, regulation of inflammation, nutrient absorption, and even prevention of infection and diseases. Some of the most common bacteria within the gut microbiome are Firmicutes, Bacteroidetes, Bifidobacteria, Proteobacteria, Verrumicrobia, Actinobacteria, Fusobacteria, and Cyanobacteria; other types of bacteria such as Actinomyces or Lactobacillus are also common in other areas of the body. All of these types of bacteria play a role in different processes that are beneficial to maintaining health. Although these microorganisms are commonly found in most individuals, each host’s microbiota is unique. Genetics, antibiotic use, diet, type of birth delivery, lifestyle, and incidence of disease can all contribute to the composition of gut microbiota.12Â Although this means that the gut microbiome is variable and certain conditions can result in dysbiosis, it is also beneficial to have the capabilities to modulate and control the gut microbiota in order to maintain healthy bodily functions and immune responses to infection.
Recently, there have been studies establishing a relationship between microbiota and cancer treatment. Particularly the gut microbiota that influences metabolic functions and inflammation and adaptive immunity play a major role in the initiation, proliferation, and response to anticancer treatment.12 In the majority of studies, the microbiota have been shown to enhance the effectiveness of cancer treatments and prolong the anticancer immune response. One way this has been demonstrated is by the transfer of faecal microbiota from mice that respond well to cancer therapy into unresponsive germ-free mice, resulting in improved anticancer reactions to treatment. Research has also shown that predictions can be made based on the patients’ gut microbiome whether or not they will have an efficient reaction to the cancer treatment or if they will exhibit negative side effects from the method of therapy.8 In addition to using the microbiome to predict patient reactions to therapy, studies have shown that it is possible to modulate the gut microbiota in order to either prevent or treat adverse effects that usually coincide with different therapies.19
These new developments are crucial for the progression of cancer therapies, especially immunotherapies. Many patients still do not respond to anticancer treatments that others do and with this promising research new opportunities for personalized therapy become an option for these individuals. Immunotherapies and modifying the microbiota of patients can offer more tailored treatment plans that can provide more promising results. In addition, these new methods can enable a more aggressive treatment plan for certain types of cancer without the fear of negative side effects or lasting damage to healthy tissue. With modulation of the microbiota, these adverse effects can be prevented and treated, using the microorganisms to protect against injury. The composition of the human microbiota plays an integral role in regulating the efficacy of anticancer treatment and development of adverse effects. (Should I include that targeting the microbiota can improve the efficacy and reduce adverse effects?
Human Microbiome and Cancer Treatments
There are many different categories of anticancer therapies, the three main types are chemotherapy, radiation therapy, and immunotherapy. However, there is interindividual variation in the gut microbiota that can determine whether the immune system is competent enough and if the patient will respond to therapy positively or negatively.19 The targeting of gut microbiota can improve the efficacy of all of these treatment plans. The figure below shows some of the processes that gut microbiota can regulate anticancer therapies.
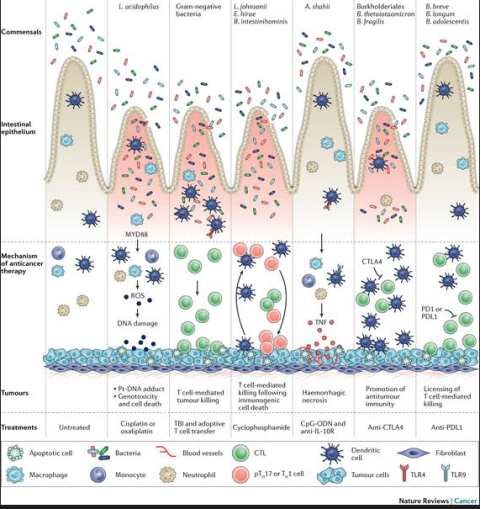
Figure 1 12
This figure is an overview of a selection of anticancer treatments that the gut microbiota can mediate or perhaps enhance… add more description…
Chemotherapy
Chemotherapy is the use of drugs, usually cytotoxic, to treat cancer. These cytotoxic drugs are typically classified according to their mechanism of action, alkylating agents, heavy metals, cytotoxic antibiotics, and spindle poisons.12 These drugs cause significant damage to any rapidly dividing cells including healthy tissues, and can therefore have varying effects on individual patients. Gastrointestinal toxicity is a common adverse effect from anticancer drugs and can be so severe that the treatment has to be postponed or the dose is limited; this reduces the efficacy of the therapy. Targeting and modifying gut microbiota can be used to protect the intestinal epithelium and prevent the toxicity of these compounds.
One mechanism of microbiota that can be exploited is its role in drug metabolism and microbial enzymatic degradation. An example of this is with the drug Irinotecan. Irinotecan is a chemotherapy drug that commonly causes severe gastrointestinal distress by increasing caecal Clostridium cluster XI and Enterobacteriaceae and cannot be used long term for treatment. SN-38, the drug’s active metabolite is converted to glucuronide which is typically cleaved by bacterial beta-glucuronidases, commonly found in the Firmicutes phylum, for a carbon source; however, this releases the active SN-38 back into the intestinal lumen leading to diarrhea.19 In this study, however, it was discovered that the bacterial enzyme has a specific loop not present in the human enzyme; this is beneficial in developing drugs to target the bacterial enzyme specifically in order to prevent the adverse effects to continue anticancer treatment. Ciprofloxacin and amoxapine were two drugs that exhibited inhibition of the bacterial enzyme, suppressing the severe diarrhea.19 The microbiota enzymatic functions can also have a role in modifying the toxic profile of chemotherapy drugs. This can cause difficulty in creating custom chemotherapy treatment plans utilizing the modulation of microbiota because some of the bacteria can have multiple effects on different targets using the same enzyme. An example of this is the bacterium Mycoplasma hyorhinis, it contains a phosphorylase that can restrict the ability to inhibit cell growth and division by drugs containing pyrimidine nucleoside. Additionally, Mycoplasma’s phosphorylase negates the efficacy of the drug gemcitabine. However, this same enzyme can improve the effectiveness of drugs containing the metabolite 5-fluoro-5′-deoxyuridine.19 This proves the difficulty in modifying each patient’s gut microbiota to improve their chemotherapeutic efficacy. Although, it can be useful and can allow the treatment plans to continue without termination due to adverse effects, it will require much more research for each individual drug’s reaction with gut microbiota enzymes. The gut microbiota can also indirectly affect the metabolism of chemo drugs through modifying gene expression and the physiology of the mucosal barrier in the intestines and liver. In one study, germ-free mice were compared with conventionally raised mice and mice given a probiotic. The germ-free mice exhibited altered gene expression to increase the rate of metabolism of many xenobiotics, whereas even after recolonization of the germ-free mice and administration of a probiotic, not all of the altered genes returned to normal gene expression.12 This raises the observation that not only does the differences in composition of microbiota and their enzyme function play a role in drug metabolism, the activity and lifestyle between individuals matters as well.
Immunomodulation and affecting the tumor-microenvironment are two additional ways that the gut microbiota have been found to modulate chemotherapeutics. Cyclophosphamide is a drug that works through many different immunological pathways, stimulating the antitumor immune response.This drug alters the composition of the microbiota in the small intestine and induces the translocation of certain gram-positive bacteria into secondary lymphoid organs.16 Once the bacteria are translocated into the lymphoid organs, they can stimulate an immune response of T helper17 cells and memory TH1 cells. The translocation of the bacteria, typically Lactobacillus johnsonii, Lactobacillus murinus, and Enterococcus hirae, takes place because cyclophosphamide causes discontinuity of the intestinal barrier allowing these microorganisms to relocate to the secondary lymphoid organs. A gram-negative bacteria, Barnesiella intestinhominis is also involved in this chemotherapy drug; it was shown to increase the systemic levels of cytotoxic CD8+ T cells and TH1 cell responses. This bacteria was also proven to activate IFNgamma-producing lymphocytes that are tumor-inflitrating.1 The role gut microbiota plays in the efficacy of cyclophosphamide treatment and immunomodulation was demonstrated by the use of germ-free mice and mice that were treated with antibiotics. The mice that were pre-conditioned with antibiotics proved to inhibit the anticancer effects of the chemotherapy drug and no reduction in the tumor size. Similarly, the germ-free mice had less pTH17 responses and their tumors were unchanged by cyclophosphamide. However, transfer of pTH17 cells restored the efficacy of the anticancer drug.1 These results show that the gut microbiota not only play a role enzymatically and through drug metabolism, but that the microbiome is used to activate the anticancer immune response. This is critical knowledge for
the progression of immunomodulation with chemotherapeutics, and gives insight as to why not all patients may react the same to this type of treatment. However, modification of the gut microbiota can enhance the efficacy and response in the patients that typically do not show change in the tumor size.
Gut microbiota can also affect the tumor microenvironment in correspondence (is that the right word?) with chemotherapeutics. Oxaliplatin and cistplatin treatments cause tumor cytotoxicity by forming intra-strand platinum-DNA adducts that lead to DNA double stranded breaks; reactive oxygen species is also involved in the damage of DNA. Although these methods are effective for creating an antitumor environment, it also causes severe damage to intestinal mucosal cells which can cause septicemia and systemic infection.12, 10 In germ-free mice the drug oxaliplatin did not induce as great of an inflammation response and consequently the antitumor efficacy was reduced, showing that inflammation is important in the drug’s antitumor response. The induced DNA damage within the tumor cells was also reduced, however oxaliplatin was still able to enter into the tumor to form fewer of the platinum-DNA adducts.16 Another effect the microbiota have on these chemo drug antitumor mechanisms was shown in germ-free mice, the production of ROS was inhibited without gut microbiota. This was previously thought to come from the cancerous cells, however the microbes prevented ROS production through tumor-infiltrating myeloid cells via NADPH oxidase 2.12 This is important to note because this shows that oxaliplatin will not be effective without gut microbiota or depleted myeloid cells. Oxaliplatin also works by inducing immunogenic cancer cell death, this can be achieved by exposing the cell surface- associated immunostimulatory signals, activating antigen-presenting cells which create and antitumor response.With a combination of activation of TLR4, DAMPs from the dying cells, and NLRP3 inflammasome, these can mediate the adaptive T cell-mediated response against the treated tumors.10 When mice are depleted of their microbiota, these cytotoxic and immunogenic effects are decreased, along with the efficacy of tumor reduction. These results demonstrate that gut microbiota can play a role in the cytotoxic effects of DNA damage and inflammation, but also can affect the adaptive immune response to cancer. Gut microbiota has an influential role in the efficacy, toxicity, and outcome of chemotherapeutics.
Radiation Therapy
Radiotherapy can consist of cancer patients receiving ionizing radiation therapy (RTX) that is typically for localized cancers, or total body irradiation (TBI) that is usually used in preparation for bone marrow transplants or adoptive T cell transfer immunotherapy. These can be effective treatment routes, however, there is a bystander effect on nearby cells that can cause inflammation, immune reactivity, and genome instability.12 These effects do not necessarily occur directly from the DNA damage caused by radiation, these typically are a result from disruption of gap junctions, and release of ROS, NO, cytokines, exosomes, and DAMP stress signals.
There are just now beginning to be more studies done about how exactly microbiota can regulate the host’s response to ionizing radiation therapy. It is difficult to study because the effects from radiation can cause a myriad of reactions within the body; some of these effects can be immunostimulating while others can be immunosuppressive. When a patient receives radiotherapy, the antitumor signals are not just contained to the localized area of the tumor; there are antitumor responses that occur that are immune mediated and activate antigen-presenting dendritic cells and T cells. Therefore, because microbiota have been shown to mediate and affect the immunogenic responses in chemotherapy and immunotherapy, it is reasonable to believe microbiota play a role in the immune system responses due to radiation. One of the major limitations to radiotherapy is the safety concern for the patient while balancing the antitumor effectiveness of receiving ionizing radiation therapy. Different cancer types will have different radiation sensitivities as well as the local and systemic toxicity and stress responses that have potential to cause significant injury or impair the antitumor immunity.12 Receiving ionizing radiation therapy is associated with damage to rapidly proliferating tissues such as epithelia, like the digestive tract mucosa, and bone marrow. These adverse effects can cause oral mucositis, diarrhea, and inflammation in the gut and can create gut microbial dysbiosis.12
A recent study investigated whether or not a faecal microbiota transplantation would protect against radiation-induced toxicity.They were able to come to the conclusion that faecal microbiota transplantation did in fact increase the survival rate of mice; in addition, the faecal microbiota transplant increased the peripheral white blood cell counts, maintained the intestinal epithelial integrity, and preserved the gut microbiota composition in mice that had been irradiated.7 Using the strategy of faecal microbiota transplantation could greatly improve the outlook for radiotherapy patients, it can reduce injury to healthy tissues and improve patients prognosis after radiotherapy.
The component that regulates irradiation-mediated intestinal toxicity is the TLR3 for double-stranded RNA. Knockout mice without Tlr3 are actually protected from TLR3-dependent cell death post radiotherapy, despite being sensitive to p53 dependent radiation-induced apoptosis. These knockout mice also survive longer and have less damaging effects on their intestines than wild-type mice. These results would suggest that blocking the TLR3 signaling could reduce the radiation-mediated gastrointestinal damage.12 In this study they also demonstrated that the DNA double stranded breaks, induced from radiation anticancer treatment, also activate a DNA receptor that is not present in melanoma 2 inflammasome; this would result in tissue damage and cell death. However, the bacterium Lactobacillus rhamnosus GG, a probiotic, has demonstrated protection of the intestinal mucosa from radiation therapy-induced toxicity. This probiotic does this by using a TLR2/MyD88 signaling mechanism to reposition cyclooxygenase 2- expressing cells from the villi to the base of the intestinal crypts which induces reactive oxygen series, leading to activation of the NRF2 system; this system is cycloprotective.6 Therefore probiotics have some capabilities to prevent radiation-induced enteropathy. The probiotic composition that studies have found to be most beneficial are Lactobacillus acidophilus, B. bifidum, Lactobacillus casei, Bifidobacterium, Lactobacillus and Streptococcus spp.5 For clinical purposes, these probiotics can be used as a prophylactic strategy to limit the intestinal injury. All of these microorganisms have been proven to protect against gut toxicity from radiation anticancer treatments; this is greatly beneficial to the patients so they do not have to endure adverse effects, such as severe diarrhea, and can continue the treatments to increase their antitumor effectiveness.
In contrast, some studies suggest that it is possible to predict whether or not a patient is going to have adverse effects to radiotherapy based off the presence of gut microbial dysbiosis or a well-balanced gut microbiome. They used pyrosequencing analysis of 16S rRNA gene to reveal the microbial diversity in the host’s gut microbiome. The individuals that had a significantly altered Firmicutes/Bacteroidetes ratio before the radiation cancer treatment, later developed diarrhea as an adverse effect from treatment. These results indicated that gut microbial dysbiosis before radiation antitumor therapy can be utilized to predict if the patient will develop adverse effects from treatment such as diarrhea.18 This knowledge could guide treatment plans to be tailored for the individual and could allow for preventative treatment options.
Total body irradiation is usually used as a preparatory process for another type of anticancer treatment such as a bone marrow transplantation or adoptive T cell transfer immunotherapy. Contrary, to the logic of many of the studies in this review, germ-free mice were shown to survive longer than conventionally raised mice after total body irradiation, and actually required a higher dosage of radiation to induce intestinal disease and mortality.7 The germ free mice were reported to have less apoptotic cells of the intestinal mucosa and even less lymphocyte infiltration than the mice with regular gut microbiota.7 They hypothesized that this could be due to the germ-free mice having no gut microorganisms that could trigger mucosal inflammation or create damage from the radiation insult. One mechanism they were able to identify that contributed to the germ-free mice resistance to total body irradiation was the production of angiopoietin-like 4. This is a protein inhibitor of lipoprotein lipase that is normally suppressed by normal gut microbiota in the conventionally raised mice.12 This angiopoietin-like 4 protein, when knocked out of germ-free mice, causes the mice to be susceptible to the same intestinal damage as conventionally raised mice that block angiopoietin-like 4 protein. Interestingly, the transcription of angiopoietin-like 4 gene is regulated in response to certain gut bacteria; however, these same bacteria that induce angiopoietin-like 4 expression include Bifidobacterium, Lactobacillus, and Streptococcus spp. that also mediate the protection against the localized received ionizing radiation therapy.12 This can provide an explanation for although most studies have shown that mice treated with probiotics and have a healthy microbiome are resistant to radiotherapy toxicity, germ-free mice can provide some resistance as well.
Although most of these studies focus on the gut microbiota, there are studies that reveal how the oral microbiota can effect prediction of enteropathy as well from radiotherapy for nasopharyngeal carcinomas. Rather than diarrhea as an adverse effect from pelvic radiotherapy, oral and oropharyngeal mucositis are the most common side effects of radiation anticancer therapy for head and neck cancers.20 Similarly to using gut microbial dysbiosis to predict whether the patient would develop adverse effects from treatment, the same can be done with analyzing the oral microbial community and its correlation with radiation-induced mucositis. The results demonstrated that patients with a higher percentage of Actinobacillus exhibited severe mucositis later on after treatment.20 Their findings also showed, similarly, that they can predict future incidence of mucositis during radiotherapy based on the oral microbiota prior to treatment. This is significant because not only can this application be applied with gut microbiota, it can be applied with the oral microbial community and many others throughout the body corresponding to different types of cancer.
Immunotherapy
Immunotherapy approaches are currently a popular topic to study and these immunological therapies have shown great potential in long-lasting responses. The efficacy of this type of treatment, however, is limited more than radiation therapy or chemotherapy because of the vast difference in immune responses of individual patients and the susceptibility of different tumor types. However, with new information about the ability of gut microbiota to modulate the host’s response to immunotherapy, it is possible to further study the possibility of improving immunotherapy efficacy by targeting these microbiota. One of the first examples of gut microbiota maintaining the anticancer effect of immunotherapy, was the demonstration that the efficacy of adoptive transfer of tumor-specific cytotoxic T cells following total body irradiation was reduced in mice treated with antibiotics.12 After the total body irradiation causes the translocation of microbiota into the secondary lymph nodes, the proliferation of the transferred T cells in the tumor and their antitumor activity was enhanced.
CpG- oligodeoxynucleotide intratumor therapy is an immunotherapy that uses the TLR9 agonist CpG- oligodeoxynucleotide to induce an antitumor effect. The antitumor effect is then increased when the immunosuppressive effect of IL-10 is prevented by using the IL-10 receptor antibodies. This method induces the secretion from myeloid cells of tumor necrosis factor and IL-12 that in turn cause hemorrhagic necrosis and can redirect tumor-infiltrating macrophages and dendritic cells from and anti-inflammatory to a pro-inflammatory state.12 There is an antigen-specific T cell antitumor that is elicited within this pro-inflammatory environment which results in the clearance of tumors in conventionally raised mice.12 This is not the case in germ-free mice or mice that have been treated with antibiotics. In these mice the tumors treated with CpG-ODNs and anti-IL-10R progress and the immunotherapy is inefficient. Finally, if the mice have a low amount of microbes, the myeloid cells do not produce pro-inflammatory cytokines and the TNF-dependent hemorrhagic necrosis and antitumor immunity are not induced.12 In these tumors, of microbiota-depleted mice, the amount of infiltrating inflammatory monocytes before treatment were unchanged but the number of Ly6C+ major histocompatibility complex class II+ were reduced. This suggests that the differentiation of infiltrating inflammatory monocytes into macrophages and dendritic cells is impaired. After CpG-oligodeoxynucleotide treatment, there are major differences in the gene expression of TNF and IL-12 in tumor-infiltrating myeloid cell subsets between microbe-depleted and conventionally raised mice.12 There is another reduction in the response to this treatment from TLR4 -deficient mice, however, treatment with the TLR4 agonist LPS to the microbe-depleted mice reinstitutes the responsiveness of the myeloid cells.12 The results from this study demonstrate that the gut microbiota primes the myeloid cells for sensitivity to TLR9. Another study using CpG-oligodeoxynucleotides showed that the CpG-ODNs correlates with the frequency of different genera in the faecal microbiome of mice at the time of treatment.12 Allistipes and Ruminococcus are positively correlated with TNF production, however, Lactobacillus fermentum, Lactobacillus murinum, and Lactobacillus intestinalis are negatively correlated, meaning when one of the bacteria from the genera Lactobacillus were administered, there was an impairment of TNF production.12 This indicates that different types of bacterial species can have opposite effects; therefore, using antibiotics, prebiotics, or probiotics, can change the gut microbiota composition or frequency resulting in mediating the host’s response to immunotherapies.
The use of immune checkpoint inhibitors is a final immunotherapy method that has been greatly studied and researched. In the majority of patients, the antitumor immune response is suppressed but can be reactivated by the release of certain signal factors. The immune checkpoint inhibitors, which are antibodies against the cytotoxic T lymphocyte-associated antigen 4 and programmed cell death protein 1 or its ligand PD1 ligand, exhibit strong antitumor activity in animal models and even long lasting clinical efficacy in cancer patients.12 Although this is a promising therapy, there is always the concern of variation of response between patients and between different types of cancers. These checkpoint inhibitors can also induce adverse effects such as colitis and inflammation of the pituitary gland in response to the cytotoxic T lymphocyte-associated antigen 4 antibodies, and thyroid dysfunction and pneumonitis after the blockade of the PDL1-PDL1 interaction.14, 15
Two recent studies investigated the influence gut microbiota has on this type of immunotherapy, specifically how anticytotoxic T lymphocyte antigen blockade requires Bacteroides spp. and how Bifidobacterium spp. enhances the effectiveness of antiprogrammed cell death ligand 1 therapy.14, 15 In the first study, in mice and patients the T cell responses specific for B. thetaiotaomicron or B. fragilis correlated with the effectiveness of CTLA-4 blockade. This was confirmed because the tumors in the germ-free mice did not respond to the CTLA blockade, but when the mice were treated with B. fragilis, this defect was overcome.15 The second study compared melanoma growth in mice with particular commensal microbiota and then observed the differences in antitumor immunity. They then sequenced the 16S ribosomal RNA which identified Bifidobacterium as associated with the antitumor effects. The administration of Bifidobacterium improved the tumor control as much as the programmed cell death protein 1 ligand 1- specific antibody treatment, and combination treatment almost ceased tumor growth.14 The results from these studies demonstrate that the mechanism of how anti-PDL1 treatment improves the antitumor immune response does not have to include microbiota inflammation and immune activation, like what is induced by anti-CTLA4. Anti-CTLA4 may alter the composition of the gut microbiota that favors its own antitumor activity. Yet, the effectiveness of the anti-PDL1 therapy is aided in hosts with a pre-existing antitumor immune response if Bifidobacterium spp. are within the gut microbiota.12
Microbiota and Lasting Effects from Treatment
After the use of cancer treatments, many times there can be lasting effects even into adulthood from childhood cancer therapies. This study demonstrated that restoring the microbial diversity in patients suffering from immune dysregulation, as a result from childhood acute lymphoblastic leukemia, could reduce chronic inflammation and reduce development of late adverse effects.4 They observed that adult survivors of childhood ALL all had microbial dysbiosis or lack of microbial diversity. The composition of host microbiota is crucial to immune activation, for example T cell activation and increased levels of IL-6 and CRP. Therefore, they hypothesized that the microbial dysbiosis was related to the background chronic inflammation in adult survivors. Additional studies would have to be performed to determine causation, but this study creates the possibility that therapeutic interventions that restore microbial diversity to the ALL survivors could help to reduce the long-term negative effects. Further research would need to be done to determine the proper mechanism to restore healthy microbial diversity to humans.
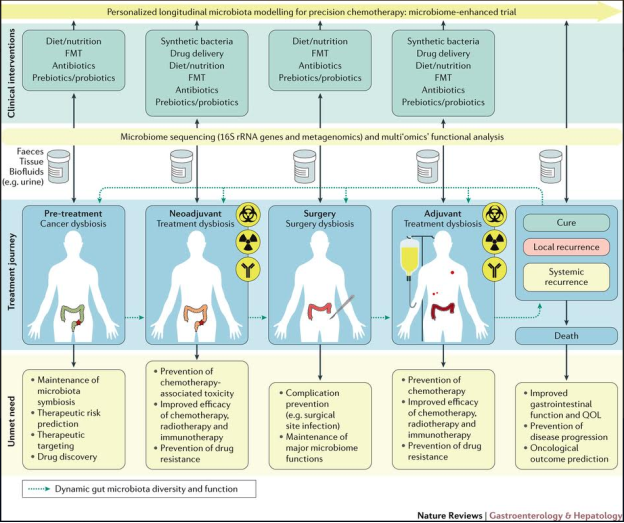
Figure 2 1
References
1. Alexander JL, Wilson ID, Teare J, Marchesi JR, Nicholson JK, Kinross JM. Gut microbiota modulation of chemotherapy efficacy and toxicity. Nature Reviews Gastroenterology & Hepatology. August 2017. doi:10.1038/nrgastro.2017.20. paper 10
2.Bultman SJ. Emerging roles of the microbiome in cancer. Carcinogenesis. 2013;35(2):249-255. doi:10.1093/carcin/bgt392. paper 17
3. Champer M, Wong AM, Champer J, et al. The role of the vaginal microbiome in gynecological cancer: a review. BJOG: An International Journal of Obstetrics & Gynaecology. 2017. doi:10.1111/1471-0528.14631. paper 9
4. Chua LL, Rajasuriar R, Azanan MS, et al. Reduced microbial diversity in adult survivors of childhood acute lymphoblastic leukemia and microbial associations with increased immune activation. Microbiome. 2017;5(1). doi:10.1186/s40168-017-0250-1. paper 7
5. Ciorba MA, Riehl TE, Rao MS, et al. Lactobacillus probiotic protects intestinal epithelium from radiation injury in a TLR-2/cyclo-oxygenase-2-dependent manner. Gut. 2011;61(6):829-838. doi:10.1136/gutjnl-2011-300367. paper 24
6. Ciorba MA, Stenson WF. Probiotic Therapy in Radiation-Induced Intestinal Injury and Repair. Annals of the New York Academy of Sciences. 2009;1165(1):190-194. doi:10.1111/j.1749-6632.2009.04029.x. paper 23
7. Cui M, Xiao H, Zhou L, et al. Faecal microbiota transplantation protects against radiation induced toxicity. EMBOpress. 2017. doi: 10.15252/emmm.201606932. paper 2
8. Dubin K, Callahan MK, Ren B, et al. Intestinal microbiome analyses identify melanoma patients at risk for checkpoint-blockade-induced colitis. Nature Communications. 2016;7:10391. doi:10.1038/ncomms10391. paper 5
9. Galloway-Pena JR, Jenq RR, Shelburne SA. Can Consideration of the Microbiome Improve Antimicrobial Utilization and Treatment Outcomes in the Oncology Patient? Clinical Cancer Research. 2017. doi:10.1158/1078-0432.ccr-16-3173. paper 8
10. Iida N, Dzutsev A, S
You have to be 100% sure of the quality of your product to give a money-back guarantee. This describes us perfectly. Make sure that this guarantee is totally transparent.
Read moreEach paper is composed from scratch, according to your instructions. It is then checked by our plagiarism-detection software. There is no gap where plagiarism could squeeze in.
Read moreThanks to our free revisions, there is no way for you to be unsatisfied. We will work on your paper until you are completely happy with the result.
Read moreYour email is safe, as we store it according to international data protection rules. Your bank details are secure, as we use only reliable payment systems.
Read moreBy sending us your money, you buy the service we provide. Check out our terms and conditions if you prefer business talks to be laid out in official language.
Read more